A Cautious Look at Japan’s Artificial Blood: Possibilities, Uncertainties, and the Unknowns
Medically Reviewed: 24th May 2026
This article has been reviewed for clinical accuracy and appropriate presentation of medical information by
Dr Muhammad Ali Fayyaz, NHS Doctor at Salford Royal Hospital, is registered with the General Medical Council UK.
Verify Active GMC Status (Ref No: 7961350)
In recent years, researchers in Japan have been working on haemoglobin vesicles, often called HbVs. These are tiny liposome-based particles made from purified and concentrated haemoglobin, the oxygen-carrying protein normally found inside red blood cells. Because they do not carry the usual red blood cell blood group markers, they may one day offer a blood-type-independent oxygen-carrying option in emergency medicine.
Although HbVs have been described as a possible universal alternative to donor blood, they remain experimental. For now, established blood conservation and transfusion avoidance strategies remain the more proven options when clinically appropriate.
What Exactly Are Haemoglobin Vesicles?
A Closer Look
Haemoglobin vesicles, often called HbVs, are tiny man-made Haemoglobin particles being developed as artificial oxygen carriers. They are designed to mimic one important function of red blood cells, carrying oxygen through the bloodstream.
They are made by taking purified and concentrated haemoglobin, the oxygen-carrying protein normally found inside red blood cells, and encapsulating it within a microscopic fatty shell called a liposome. In current research, this haemoglobin is sourced from donated human red blood cell concentrate that has been screened and processed, including material that may otherwise be discarded.
Because HbVs lack the usual red blood cell blood group markers on their surface, they may be used without the ABO blood group matching required for ordinary red blood cell transfusions. However, they remain under clinical investigation and would need full regulatory approval before routine hospital use.
It is also important to be clear that HbVs are not truly blood-free. Although the outer capsule is man-made, the haemoglobin inside is derived from human blood. The manufacturing process includes extensive screening, purification, and viral reduction steps designed to greatly reduce infectious risk, but the human blood origin remains an important detail.
For anyone seeking treatment options that avoid human blood derived components, this distinction could be very important.
Helpful Definitions
- ABO Compatibility: HbVs do not carry the usual red blood cell surface antigens, so they are being developed as a blood type independent oxygen carrier. This could reduce the need for ABO matching, although clinical suitability would still depend on the patient and the approved use.
- Half-Life: HbVs appear to work as short term oxygen carriers, with a circulation time measured in hours. This could make them useful as an emergency bridge, but they are not like standard donated red cell units, which can be stored for several weeks before transfusion, around 35 days in the UK and up to 42 days in some other systems.
- P50 Value: This shows how well haemoglobin lets oxygen go to tissues. HbVs are designed to behave like natural red blood cells (~30 Torr).
Where It Could Help — But with Caveats
HbVs are envisioned to assist in:
- Disaster zones where refrigeration and blood typing are tough.
- Military or rescue missions, where rapid, universal help is vital.
- Remote clinics without cold storage.
Yet, remember:
- It’s a stop-gap, not a complete replacement.
- We’ve only seen limited human trials — no long‑term data.
- Production could be expensive and challenging.
- HbVs cannot clot blood, replace platelets or plasma, support immune function, or fully replace the many roles of whole blood.
The Development Journey
- 2022: Small safety trial (100 mL doses) in healthy volunteers, no major concerns.
- 2025: Phase 1 extended to 16 volunteers (up to 400 mL), safety still reassuring.
- 2025–26: Larger Phase 2/3 trials expected.
- 2030 or later: If all goes well, HbVs might reach hospitals, but timelines could slip.

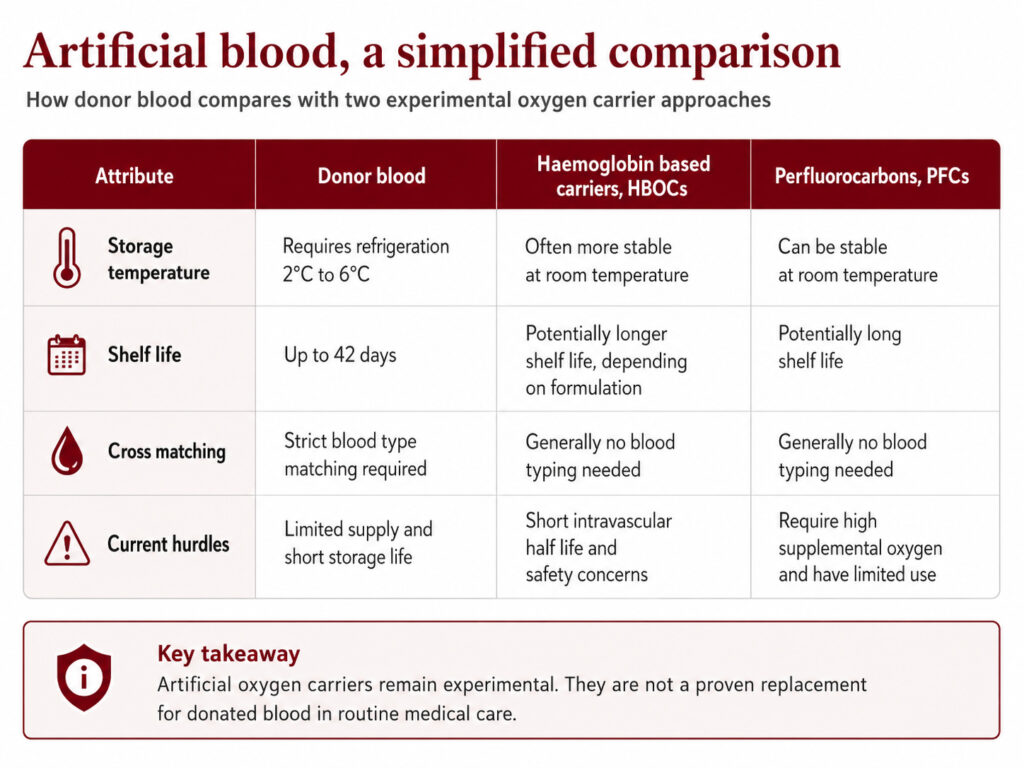
How Do HbVs Achieve? — A Quick Comparison

Lessons from the Past
Earlier artificial blood efforts (like PolyHeme or perfluorocarbons, acellular chemically modified HBOCs) failed due to short lifespan, side effects (statistically higher risks of myocardial infarction/cardiovascular events and death) or breakdown. HbVs aim to learn from those mistakes, but the proof of success is still ahead.
What We Don’t Yet Know
- How will HbVs respond in complex cases, such as surgery or chronic anaemia?
- What about repeated doses over time?
- Can manufacturers scale up production affordably?
- Will regulators in countries outside Japan approve them?
- How cost-effective would this be?
With these uncertainties, it’s wise to remain realistic.
Could HbVs be acceptable to people who refuse blood transfusions?
Because HbVs contain haemoglobin derived from human blood, they may raise important personal, religious, or ethical questions for people who refuse blood or blood-derived products. Acceptance would depend on the individual’s own beliefs, medical advice, and informed consent.
How far are we from HBVs being proven and used as a safer product with controlled side effects?
Because Some Tools Are Proven and Already Here
While HbVs are being developed, there’s no need to wait for something untested. Multiple already‑available alternatives have strong safety records:
- Cell salvage systems: collect and return your own blood during surgery.
- Volume expanders: saline, colloids or other fluids that support circulation.
- Pre‑operative autologous donation: storing your own blood before planned surgery.
- Acute normovolaemic haemodilution: remove and later return some of your blood during surgery.
- Erythropoiesis‑stimulating drugs and iron therapy: boost red cell production over weeks.
- Tranexamic acid and other agents: help stop bleeding during and after surgery.
Major hospital blood management programmes have shown that these methods can reduce reliance on transfusion when used appropriately.
Final Thoughts
HbVs are intriguing, and could one day help fill gaps when supplies, refrigeration or blood matching aren’t options. But at present, they’re unproven, limited, and expensive.
For now, if you’re concerned about transfusions or want to avoid them, established alternatives offer reliable, well‑tested safety. Innovation inspires hope, but when lives are at stake, evidence is everything. Until HbVs have that, we should trust what we already know works.
To ensure your treatment preferences are legally protected in an emergency, you can follow our complete guide on how to create an Advance Decision in the UK.
Medical Review, Disclosure and Disclaimer
Medical Reviewed: 24th May 2026
This article has been independently reviewed for clinical accuracy, patient safety and appropriate presentation of medical information by Dr Muhammad Ali Fayyaz, NHS Doctor at Salford Royal Hospital, who is registered with the
General Medical Council UK.
Dr Muhammad Ali Fayyaz was compensated by My Medical Choice for his time and professional input.
This article is for general educational purposes only and should not be treated as personal medical or legal advice. Readers should consult their own healthcare team, GP, consultant, or a suitably qualified legal professional regarding their individual circumstances, treatment options, emergency care planning, advance care planning, and any questions about blood products or blood alternatives.
Verify Dr Muhammad Ali Fayyaz’s active GMC status
(Ref No: 7961350)
Written by Giovanni Castagno, contributing writer for My Medical Choice, with several years of experience creating educational healthcare content to support patient rights and future planning in the UK.
Looking for recognised options that may help you plan safer treatment choices today?
While artificial blood remains experimental, many established options already exist to reduce or avoid transfusions. From cell salvage to iron therapy, these methods are helping thousands of patients every year. Discover blood transfusion alternatives.
See our Clinically Reviewed Guides
* Medical guidance changes over time. This article is periodically reviewed and updated to help ensure the information remains accurate and reflects current UK guidance where applicable.
Source: